Post Disclaimer
This post contains affiliate links. If you buy something through these links, I may earn a small commission at no extra cost to you. Full disclosure.
This article is for informational purposes only and does not constitute medical advice. Always consult a healthcare professional for personal health concerns. Full disclaimer.
Last updated: June 26, 2026
Quick Answer: Insomnia in children is more common than most parents expect – affecting an estimated 20-30% of kids at some point during childhood [7]. It shows up as difficulty falling asleep, frequent night waking, or waking too early and being unable to get back to sleep. The good news is that most cases respond well to behavioral approaches, and medication is rarely the first or best answer.
Key Takeaways
- Insomnia in children looks different from adult insomnia – kids often don’t recognize they have a problem, and behavior changes are usually the first clue
- The most common signs are bedtime resistance, frequent night waking, and daytime irritability or difficulty concentrating
- Anxiety, ADHD, inconsistent routines, and screen exposure before bed are among the leading causes
- Sleep needs vary significantly by age – a 5-year-old needs roughly 10-13 hours; a teenager needs 8-10
- Cognitive Behavioral Therapy for Insomnia (CBT-I) adapted for children is the most evidence-backed non-medication approach [7]
- Melatonin can be useful short-term but is not well-studied for long-term use in children – talk to a pediatrician first
- Most parents unknowingly reinforce sleep problems through well-meaning habits like staying until the child falls asleep
- If sleep problems persist beyond 3-4 weeks and affect daytime functioning, it’s time to see a doctor [2]
What Is Insomnia in Children and How Is It Different From Adults
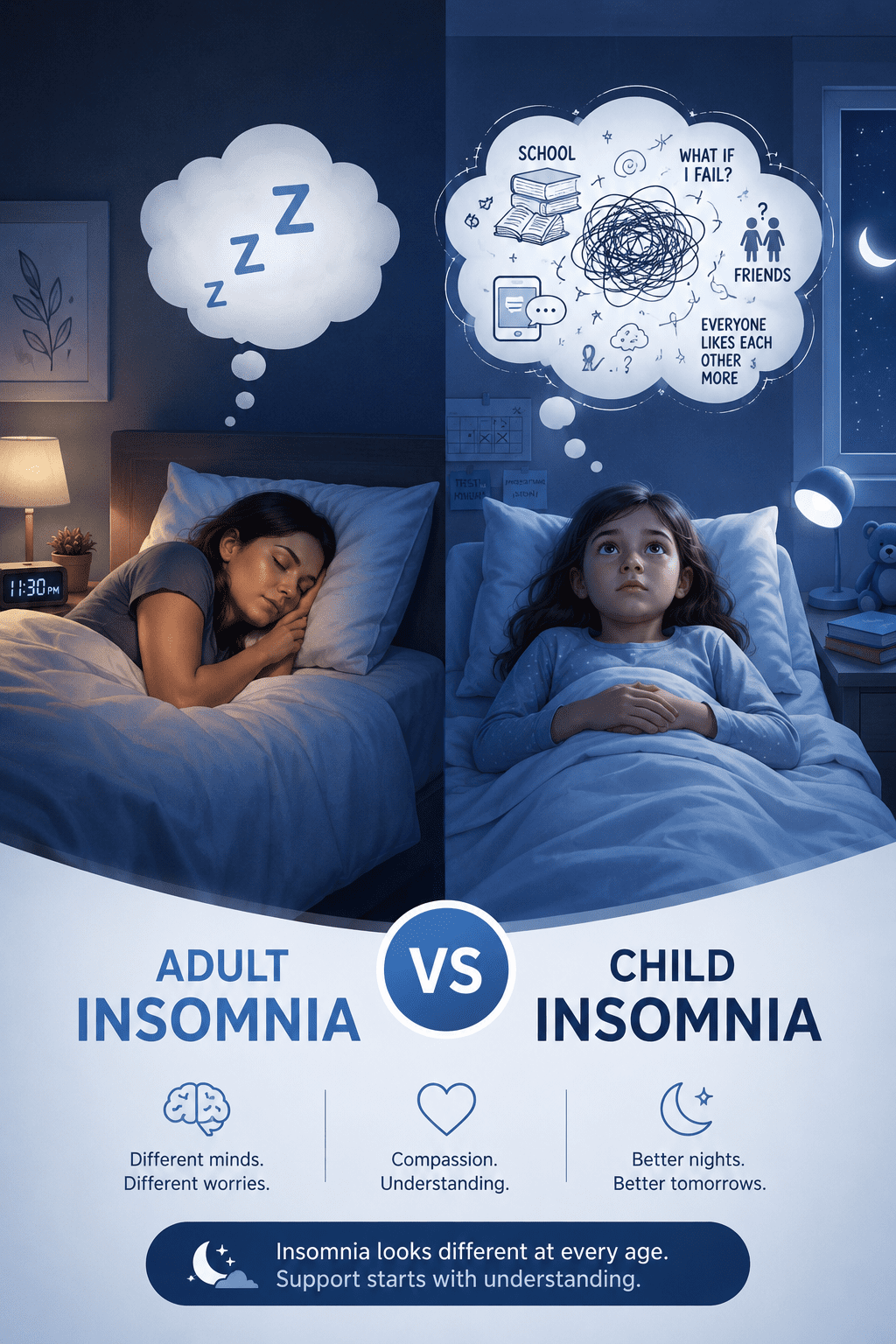
Insomnia in children is defined as repeated difficulty falling asleep, staying asleep, or waking too early – despite having enough opportunity and a safe environment to sleep. The key difference from adult insomnia is that children rarely self-report it. They don’t come to you and say “I have insomnia.” Instead, you see it in their behavior.
Adults with insomnia usually know they have a problem. They lie awake worrying about not sleeping. Children, especially younger ones, don’t have that self-awareness. What you get instead is a child who fights bedtime, cries when you leave the room, or shows up in your bed at 2am. The sleep problem expresses itself through behavior, not complaint.
Another difference worth knowing: children’s sleep architecture changes dramatically across development. A toddler’s sleep cycle is not the same as a teenager’s, and what counts as a problem at age 4 may be completely normal at age 14. Context matters a lot here.
Research also shows that children who experience insomnia are at higher risk of developing persistent sleep problems into adulthood [6]. That’s not meant to alarm you – it’s meant to make the case that taking it seriously now is worth it.
What Are the Signs That My Child Has Insomnia
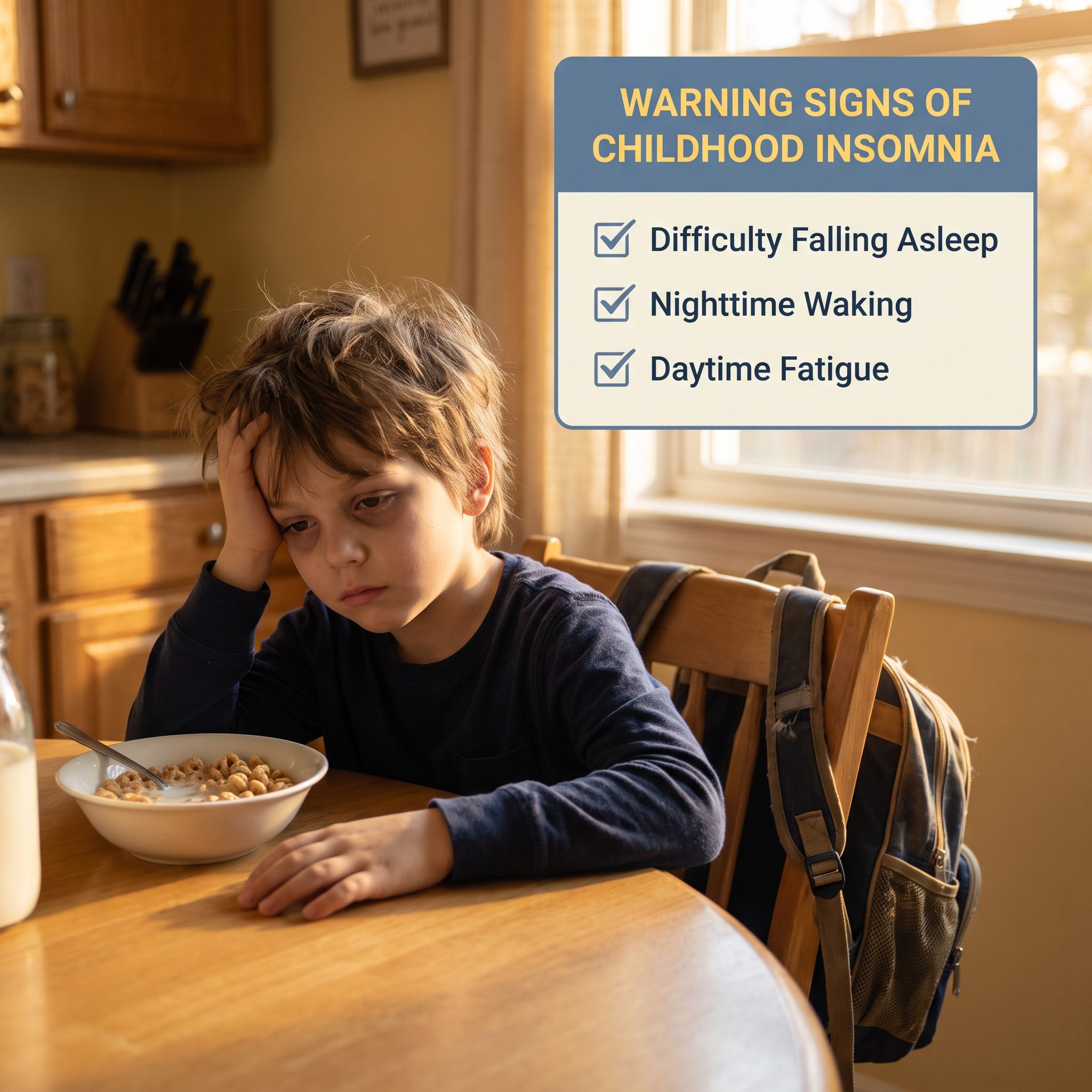
The clearest signs are behavioral, not verbal. A child with insomnia typically shows one or more of the following:
- Takes more than 20-30 minutes to fall asleep most nights
- Wakes frequently during the night and can’t resettle without a parent
- Wakes very early and can’t go back to sleep
- Resists bedtime strongly and consistently – not just occasionally
- Seems exhausted during the day but still can’t sleep at night
- Has difficulty concentrating at school or becomes unusually irritable or emotional
Daytime function is actually one of the most important markers [2]. A child who sleeps poorly but seems fine during the day is a different situation from a child whose school performance, mood, or social behavior is visibly affected. The honest version is: if it’s affecting their days, it’s worth addressing.
I’ve noticed that parents often normalize these signs for months before connecting them to sleep. The irritability gets blamed on personality. The school struggles get blamed on the teacher. It’s not always obvious that the root issue is sleep.
If you’re seeing these signs consistently for more than 2-4 weeks, consider taking this free anonymous sleep assessment to get a clearer picture of what’s going on:
Take the free insomnia assessment here – it evaluates how you’ve been feeling over the past two weeks and takes just a few minutes.
Why Do Children Develop Insomnia
Insomnia in children rarely has a single cause. It’s usually a combination of factors that build on each other.
The most common causes include:
- Anxiety and stress – school pressure, social problems, family changes like divorce or a new sibling
- Inconsistent sleep schedules – different bedtimes on weekdays vs. weekends create a kind of social jet lag
- Sleep associations – when a child has only ever fallen asleep with a parent present, they can’t resettle alone when they naturally wake at night
- Medical issues – sleep apnea, restless legs syndrome, and chronic pain can all disrupt sleep [7]
- Screen exposure – blue light and stimulating content before bed suppress melatonin and delay sleep onset [9]
- Caffeine – more common than parents realize, through sodas, energy drinks, and even some teas
- Neurodevelopmental conditions – ADHD and autism spectrum disorder have high rates of co-occurring sleep problems [5]
For a broader look at what drives sleep disruption across all ages, the article on surprising insomnia causes beyond stress covers several factors that apply to children too.
How Much Sleep Does My Child Actually Need by Age
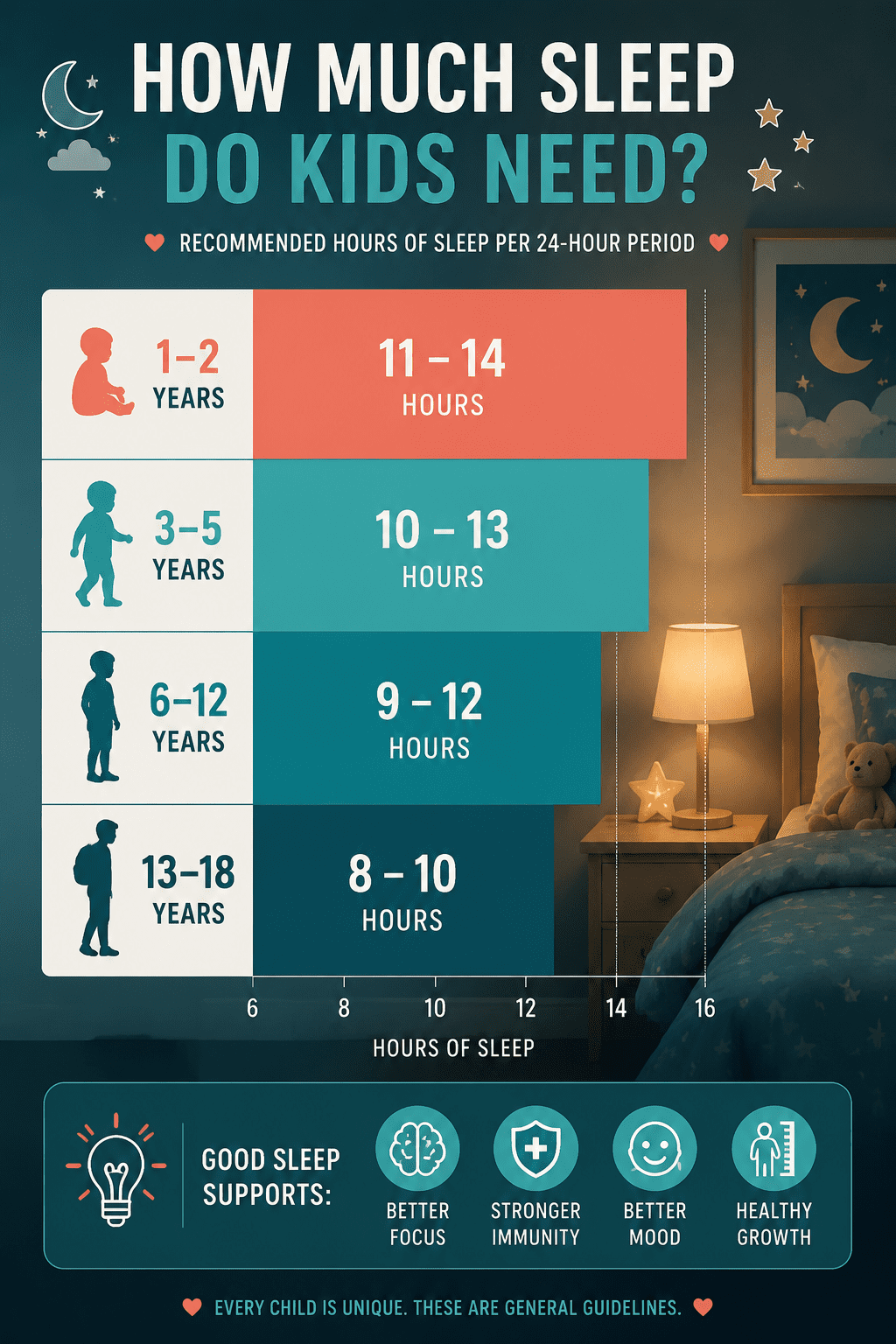
Sleep needs aren’t one-size-fits-all, and they change significantly as children grow. Here are the American Academy of Sleep Medicine guidelines, as cited by the Sleep Foundation and NIH:
| Age Group | Recommended Sleep (per 24 hours) |
|---|---|
| Infants (4-12 months) | 12-16 hours (including naps) |
| Toddlers (1-2 years) | 11-14 hours (including naps) |
| Preschool (3-5 years) | 10-13 hours (including naps) |
| School age (6-12 years) | 9-12 hours |
| Teenagers (13-18 years) | 8-10 hours |
In practice, this means a 7-year-old who goes to bed at 9pm and wakes at 6am is getting 9 hours – technically within range, but on the low end. If that same child is struggling to fall asleep until 10pm, they’re running a real deficit.
Worth noting: teenagers have a biological shift in their circadian rhythm that makes them naturally want to sleep and wake later. This isn’t laziness or defiance. It’s physiology. Forcing an early bedtime on a 16-year-old often backfires.
What Causes Insomnia in Kids With Anxiety or ADHD
Children with anxiety or ADHD have significantly higher rates of insomnia than the general pediatric population [5]. For kids with anxiety, the bedroom becomes a place where worries feel louder – there’s no distraction, no activity, just thoughts. The racing mind at bedtime that adults with insomnia know so well? Kids with anxiety experience the exact same thing.
For children with ADHD, the mechanisms are different. ADHD is associated with delayed circadian rhythms, difficulty transitioning from high stimulation to rest, and in many cases, the stimulant medications used to treat ADHD can directly interfere with sleep onset [5].
If your child has either condition, treating the sleep problem in isolation often doesn’t work. The underlying anxiety or attention issues need to be part of the picture. A pediatric psychologist or sleep specialist who understands both is worth seeking out.
This is also where the insomnia and overthinking connection becomes relevant – the same cognitive patterns that keep adults awake apply to older children and teens.
Can Screen Time Before Bed Cause Insomnia in Kids
Yes, and here’s what the research actually says: screens before bed affect children’s sleep through two pathways. First, the blue light emitted by phones, tablets, and TVs suppresses melatonin production, which delays the natural sleep signal [9]. Second, and arguably more important, stimulating content – games, videos, social media – keeps the brain in an activated state that’s incompatible with sleep onset.
A 2016 study published in Nature found significant associations between screen use at bedtime and shorter sleep duration and later sleep timing in children [9]. More recent research continues to support this relationship.
The practical takeaway: screens off at least 60 minutes before bed is the standard recommendation. For kids who are already struggling with sleep, 90 minutes is better. The reason this matters is not just the light – it’s the mental arousal. A child who just finished a competitive video game is not in a physiological state ready for sleep, regardless of how tired they feel.
That said – I know telling a parent to enforce a screen cutoff sounds obvious, and it’s not always easy. The key is making it a non-negotiable part of the routine, not a nightly negotiation.
How Do I Help My Child Fall Asleep Naturally Without Medication
Behavioral approaches are the most effective and most durable interventions for childhood insomnia [7]. The goal is to teach the child’s nervous system that the bedroom is a safe, predictable place for sleep – and that they can fall asleep independently.
The core strategies:
- Consistent sleep and wake times – including weekends. This anchors the circadian clock.
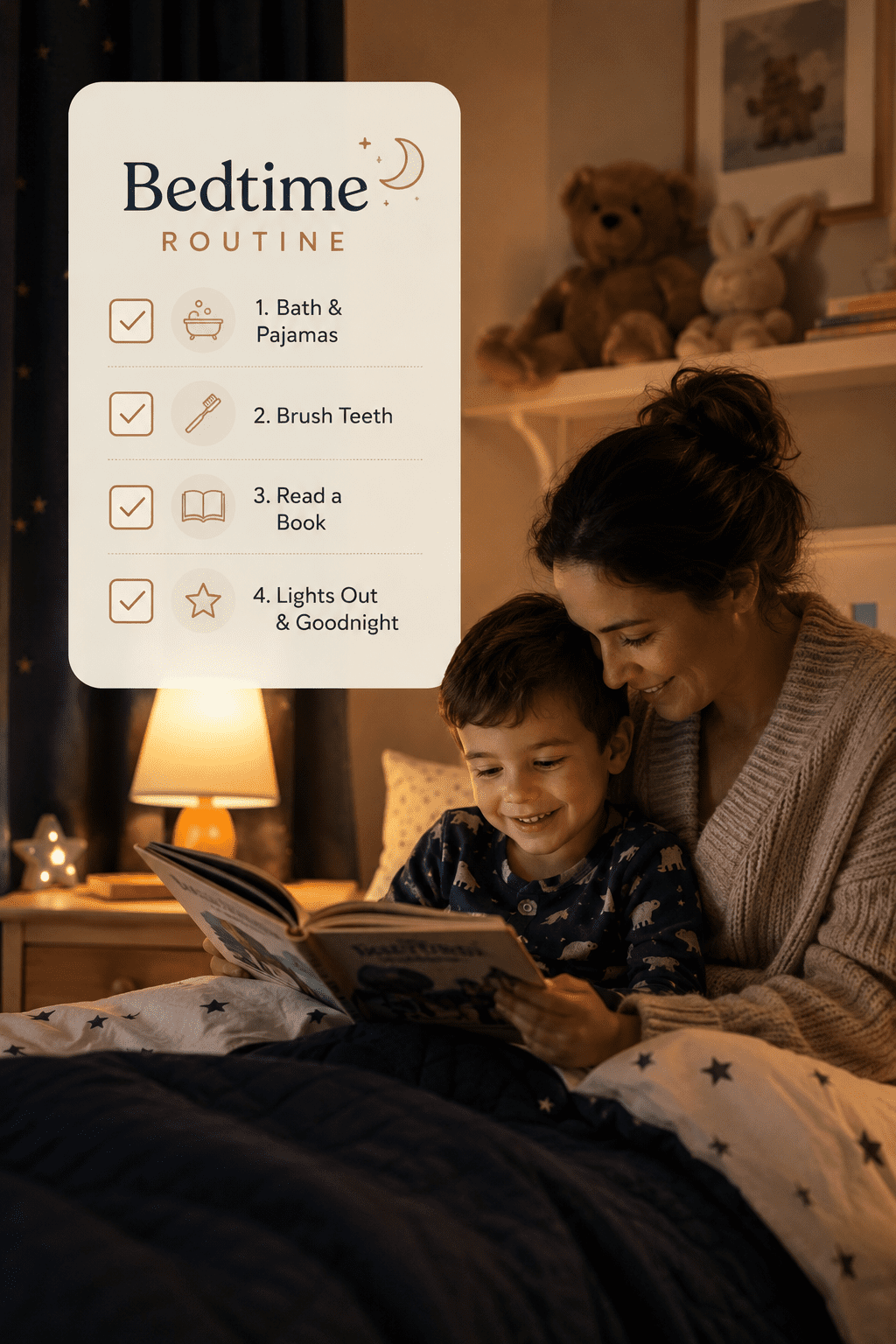
- A predictable wind-down routine – 20-30 minutes of calm activity before bed. Bath, book, quiet conversation. Same order, every night.
- Teach independent sleep onset – the child should fall asleep in their own bed, not in your arms or with you present. This is the single most important factor in preventing night waking.
- Limit stimulating activities in the hour before bed – screens, rough play, anything that raises heart rate or mental arousal
- Keep the bedroom cool, dark, and quiet – basic but genuinely effective
For older children and teens, relaxation techniques like slow breathing or progressive muscle relaxation can help. These aren’t magic, but they give the child something to do with their body instead of lying there fighting sleep.
You don’t have to fall asleep – you just have to rest. Teaching this mindset to an anxious child can reduce the performance pressure around sleep that makes insomnia worse.
For more on building a routine that actually sticks, the bedtime routine guide for adults has principles that translate directly to older kids and teens.
What Are Common Mistakes Parents Make With Kids’ Bedtime Routines
Most parents who struggle with a child’s sleep are doing something that works in the short term but makes the problem worse over time. It’s not bad parenting – it’s a natural response to a distressed child.
The most common mistakes:
- Staying until the child falls asleep – this creates a sleep association where the child can only fall asleep with you present. When they naturally wake at 2am, they need you again.
- Inconsistent responses to night waking – sometimes going in immediately, sometimes waiting. Inconsistency actually increases anxiety and prolongs the problem.
- Bedtime that’s too late – overtired children often have more trouble falling asleep, not less. An earlier bedtime frequently helps.
- Letting weekends run wild – sleeping in 2-3 hours on weekends shifts the internal clock and makes Sunday night a guaranteed struggle.
- Using screens as a wind-down tool – it feels calming but it isn’t, physiologically speaking.
Worth trying if your child is school-age or older: involve them in designing the bedtime routine. Children who have some ownership over the process tend to resist it less.
Is Melatonin Safe for Children With Insomnia
Melatonin is widely used for children’s sleep problems, but “widely used” doesn’t automatically mean “well-studied for long-term use.” Here’s what the evidence actually supports: melatonin can help shift sleep timing – it’s most useful for children whose internal clock is running late, causing them to fall asleep too late and wake too late. It’s also used in children with ADHD or autism, where there’s more research support [7].
For children with behavioral insomnia – the kind caused by poor sleep associations or anxiety – melatonin addresses the symptom but not the cause. The behavioral work still needs to happen.
The honest version is: short-term melatonin use under pediatric guidance appears to be safe for most children, but it shouldn’t be the first tool you reach for, and it shouldn’t replace addressing the underlying issue. Talk to your child’s doctor before starting it – dosing matters, and the supplement market is not well-regulated.
Medical disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before starting any supplement or treatment for your child.
What Is the Difference Between Insomnia and Just Being a Light Sleeper
A light sleeper wakes easily but falls back asleep without difficulty and functions well during the day. Insomnia involves difficulty falling asleep, staying asleep, or both – and the key marker is daytime impairment [2].
If your child wakes at small sounds but settles within minutes and isn’t tired or irritable the next day, that’s likely just their natural sleep style. If waking leads to prolonged difficulty resettling, and the next day is affected, that’s closer to insomnia territory.
The clinical threshold used by sleep researchers is: sleep difficulty occurring at least 3 nights per week, for at least 3 months, with associated daytime dysfunction [1]. Before that point, it may be a temporary disruption rather than true insomnia.
When Should I Take My Child to a Doctor for Sleep Problems
If sleep problems have persisted for more than 3-4 weeks, are happening most nights, and are affecting your child’s daytime functioning – school, mood, behavior, growth – it’s time to involve a professional [2].
You should also seek medical evaluation sooner if you notice:
- Loud snoring, gasping, or pauses in breathing during sleep (possible sleep apnea)
- Your child complains of uncomfortable sensations in their legs at night (possible restless legs)
- Significant behavioral changes alongside the sleep problems
- The child is very young (under 2) and sleep disruption is severe
A pediatrician is a good starting point. For persistent or complex cases, a referral to a pediatric sleep specialist or a child psychologist trained in CBT-I is worth asking for.
If you’re unsure whether what you’re seeing crosses the threshold for a real problem, this free anonymous test can help clarify things:
Take the free insomnia assessment – it’s designed to evaluate sleep-related symptoms over the past two weeks and takes only a few minutes.
Are There Behavioral Techniques Instead of Medication for Child Insomnia
Yes – and they work better than medication for most children. Cognitive Behavioral Therapy for Insomnia (CBT-I), adapted for pediatric use, is the most evidence-backed approach available [7]. It addresses the thoughts, behaviors, and environmental factors that maintain insomnia – rather than just sedating the child.
For younger children, behavioral approaches focus on parents: establishing consistent routines, modifying how they respond to night waking, and gradually reducing the child’s dependence on parental presence to fall asleep.
For older children and teens, CBT-I techniques include sleep restriction (temporarily limiting time in bed to build sleep drive), stimulus control (using the bed only for sleep), and cognitive work to address anxious thoughts about sleep.
Digital tools delivering CBT-I content have also shown promising results in pediatric populations globally [8]. These aren’t a replacement for professional support in complex cases, but they can be a useful starting point.
For parents dealing with their own sleep struggles alongside their child’s, the guide on insomnia solutions for the last hour before bed and the 15 insomnia tips that actually work are worth reading too.
How Long Does It Take to Fix a Child’s Sleep Schedule
For behavioral insomnia in children, consistent application of the right strategies typically produces noticeable improvement within 2-4 weeks [7]. Full resolution – meaning the child falls asleep independently and sleeps through most nights – often takes 4-8 weeks.
The catch is consistency. Partial implementation, or giving in on hard nights, resets the clock. This is the part most parents find genuinely difficult, and it’s okay to acknowledge that.
If you’ve been dealing with this for a while and nothing seems to stick, it may be worth looking at whether there’s an underlying issue – anxiety, a medical condition, or a sleep association that hasn’t been fully addressed – rather than trying yet another routine tweak.
For practical guidance on resetting a sleep schedule, the step-by-step guide to fixing your sleep schedule in 7 days has a framework that can be adapted for older children and teens.
Conclusion
Insomnia in children is real, it’s common, and it’s not something your child will necessarily just grow out of without some intervention. The research is clear that untreated childhood sleep problems carry forward [6] – but the research is equally clear that behavioral approaches work, and work well [7].
Here’s what to do next:
- Track your child’s sleep for one week – bedtime, wake time, night wakings, and daytime mood. Patterns become visible quickly.
- Audit the bedtime routine for the common mistakes above – inconsistency, screens, late bedtimes, and parental sleep associations.
- If anxiety or ADHD is in the picture, address those alongside the sleep work – not separately.
- If problems persist beyond 3-4 weeks with real daytime impact, talk to your pediatrician and ask specifically about CBT-I referrals.
- If you’re not sure whether what you’re seeing is a real problem, take the free anonymous insomnia assessment – it takes a few minutes and gives you a clearer baseline.
It’s not just you. Sleep problems in families are exhausting in a way that’s hard to explain to someone who hasn’t lived it – because you’re dealing with a sleep-deprived child while being sleep-deprived yourself. Start with one change, hold it consistently for two weeks, and see what moves.
FAQ
Q: Can a 3-year-old have insomnia?
Yes. Behavioral insomnia is actually most common in toddlers and preschoolers. It typically involves difficulty falling asleep alone or frequent night waking that requires parental intervention.
Q: My child falls asleep fine but wakes at 3am every night. Is that insomnia?
It can be. Frequent night waking with inability to resettle independently is one of the recognized presentations of childhood insomnia, especially when it causes daytime impairment.
Q: Should I let my child cry it out if they have insomnia?
Graduated extinction (controlled crying) is one evidence-based approach for younger children, but it’s not the only option and isn’t appropriate for all ages or situations. For older children, behavioral approaches that involve the child are more effective.
Q: Can diet affect my child’s sleep?
Yes. Caffeine – found in sodas, energy drinks, and some teas – is a common and overlooked culprit. Heavy meals close to bedtime and low magnesium intake have also been associated with sleep disruption.
Q: Is it normal for teenagers to have trouble sleeping?
Teenagers have a biological circadian shift that pushes their sleep timing later. Combined with early school start times, this creates a structural sleep deficit for many teens. It’s not purely behavioral.
Q: What’s the youngest age at which melatonin is considered?
Most pediatric guidelines suggest melatonin is not appropriate for children under 3 without medical supervision. For older children, it should be used under pediatric guidance, at low doses, and not as a long-term solution.
Q: Can a child’s insomnia affect the whole family’s sleep?
Absolutely – and this is underappreciated. Parents of children with insomnia report significantly disrupted sleep themselves, which affects their own functioning and patience. Addressing the child’s sleep is also addressing the family’s sleep.
Q: Does napping make childhood insomnia worse?
For school-age children and teens, daytime napping can reduce sleep pressure and make nighttime sleep harder. For toddlers and preschoolers, age-appropriate naps are still necessary and shouldn’t be cut prematurely.
References
[1] pubmed.ncbi.nlm.nih.gov – https://pubmed.ncbi.nlm.nih.gov/41478207/
[2] Improving Sleep Isn’t Enough: Researchers Highlight Daytime Function As Key To Assessing Insomnia Treatments – https://www.medschool.umaryland.edu/news/2026/improving-sleep-isnt-enough-researchers-highlight-daytime-function-as-key-to-assessing-insomnia-treatments.html
[5] S0149763422001427 – https://www.sciencedirect.com/science/article/abs/pii/S0149763422001427
[6] Study: Children with Insomnia at Higher Risk for Sleep Problems as Adults – https://www.nhlbi.nih.gov/news/2022/study-children-insomnia-higher-risk-sleep-problems-adults
[7] PMC7953218 – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7953218/
[8] Digital Tools Show Global Promise For Helping Young Children Sleep Better – https://news.med.miami.edu/digital-tools-show-global-promise-for-helping-young-children-sleep-better/
[9] Srep27921 – https://www.nature.com/articles/srep27921