Post Disclaimer
This post contains affiliate links. If you buy something through these links, I may earn a small commission at no extra cost to you. Full disclosure.
This article is for informational purposes only and does not constitute medical advice. Always consult a healthcare professional for personal health concerns. Full disclaimer.
Last updated: June 8, 2026
Quick Answer: Insomnia is rarely one thing. Most people who ask “why do I have insomnia” are dealing with a combination of triggers — stress, an underlying medical condition, disrupted sleep schedules, or habits that quietly wreck sleep quality over time. Figuring out your specific trigger is the first step toward actually fixing it, and it matters more than any sleep tip you’ll find on a list.
Key Takeaways
- Insomnia is a symptom, not a disease — something is causing it, and that cause is findable
- Stress and anxiety are the most common triggers, especially for sudden-onset insomnia
- Chronic insomnia (lasting more than three months) carries real health risks and usually needs more than sleep hygiene fixes
- Medical conditions — thyroid issues, sleep apnea, chronic pain — are frequently missed as causes
- Some medications directly disrupt sleep as a side effect
- Diet, alcohol, and irregular schedules affect sleep more than most people realize
- Insomnia can be a sign of depression or anxiety — the relationship runs both ways
- Keeping a sleep diary for two weeks is the most practical first step for identifying your trigger
- CBT-I (Cognitive Behavioral Therapy for Insomnia) is the most evidence-backed treatment for chronic cases
- If you’ve been struggling for more than a month, it’s worth talking to a doctor
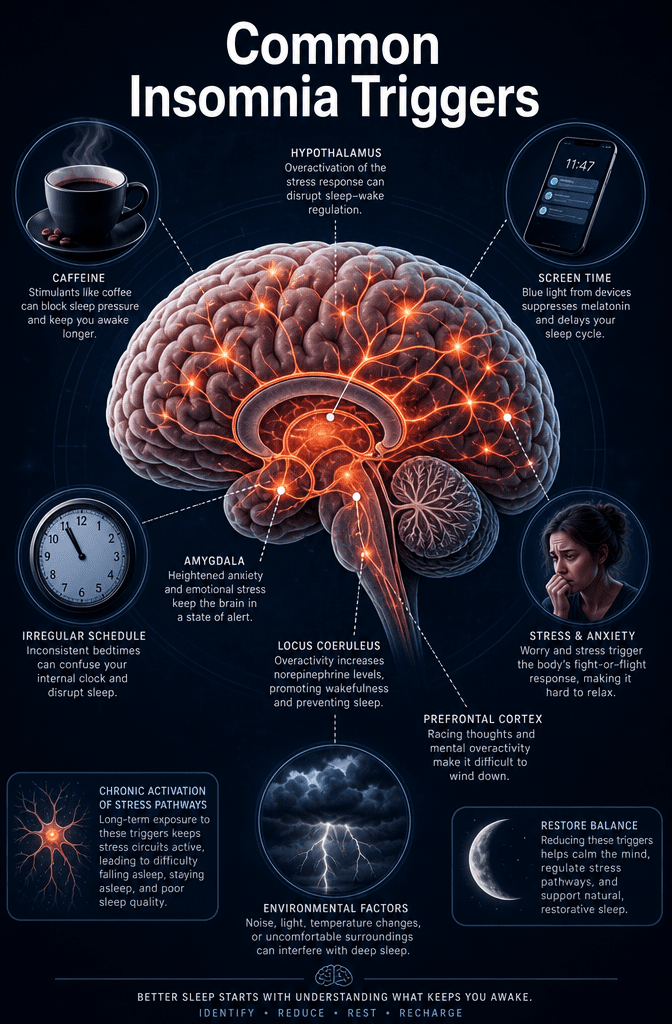
What Are the Most Common Causes of Insomnia?
Insomnia has a short list of usual suspects, and most cases trace back to one or more of them. According to the Sleep Foundation, the main categories are psychological factors (stress, anxiety, depression), lifestyle habits, medical conditions, medications, and circadian rhythm disruption [4].
Here’s what the research actually says: no single cause dominates. Most people dealing with chronic sleeplessness have a primary trigger that opened the door — a stressful event, a health change, a new medication — and then a set of learned behaviors that kept the insomnia going long after the original trigger faded.
The most common causes, in plain terms:
- Stress and worry — work pressure, relationship problems, financial anxiety, grief
- Anxiety disorders — generalized anxiety, panic disorder, PTSD
- Depression — both a cause and a consequence of poor sleep
- Poor sleep habits — irregular bedtimes, long naps, too much time in bed awake
- Stimulants — caffeine, nicotine, certain medications
- Alcohol — disrupts sleep architecture even if it helps you fall asleep initially
- Medical conditions — chronic pain, asthma, acid reflux, thyroid disorders, sleep apnea
- Circadian rhythm disruption — shift work, jet lag, irregular schedules, late-night light exposure
- Hormonal changes — menopause, pregnancy, thyroid fluctuations [1][4]
If you’ve been dealing with this for a while, the honest version is that you probably already know which category fits — you just haven’t connected it clearly yet.
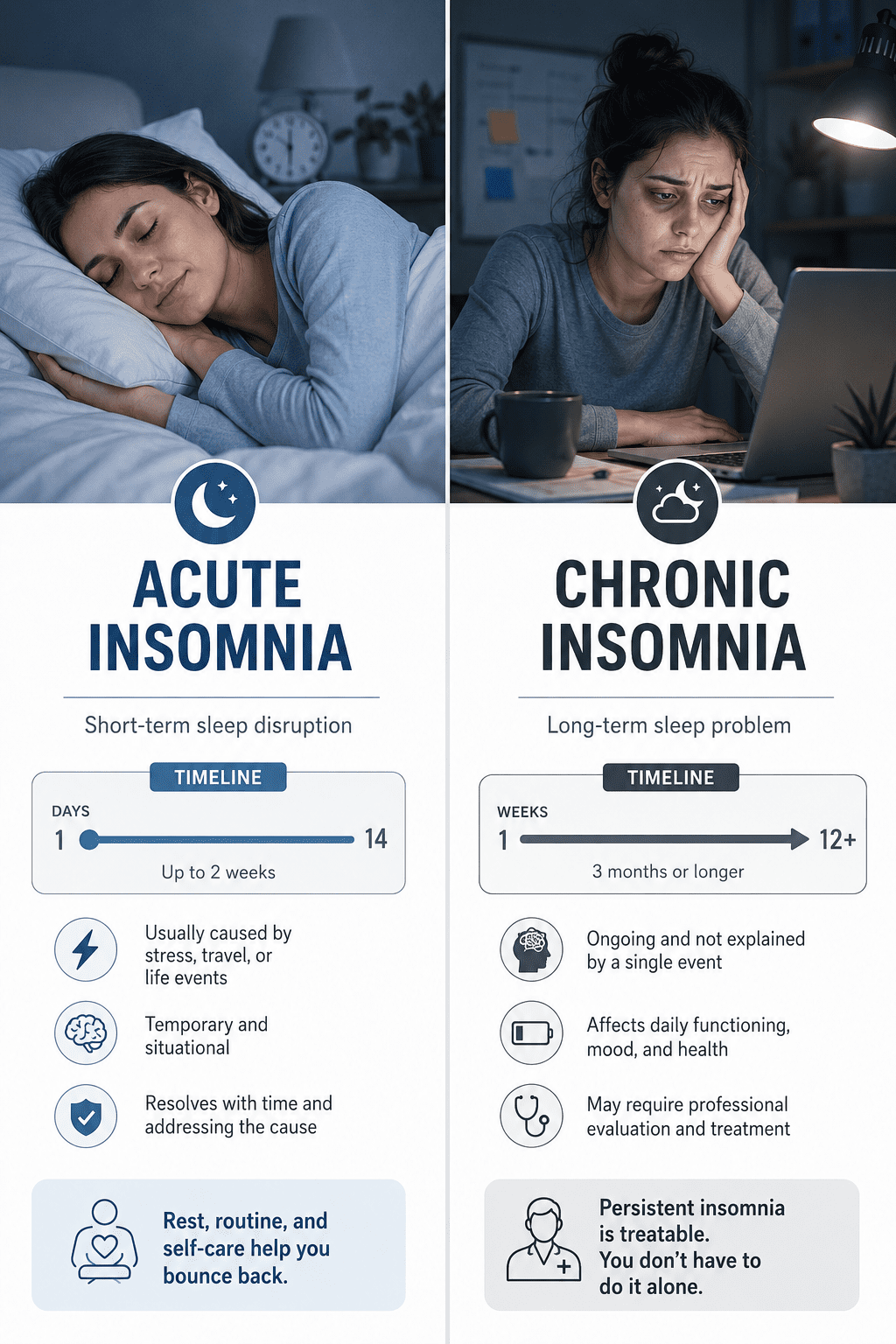
What’s the Difference Between Acute and Chronic Insomnia?
Acute insomnia is short-term — it lasts days to a few weeks and is usually tied to a specific event or stressor. Chronic insomnia means you’re having trouble sleeping at least three nights per week for three months or more [10].
This distinction matters because the approach is different. Acute insomnia often resolves on its own once the trigger passes. Chronic insomnia usually doesn’t — it tends to develop a life of its own, driven by anxiety about sleep itself and habits that reinforce wakefulness. The Mayo Clinic notes that chronic insomnia may require treatment to address both the sleep problem and whatever is sustaining it [1].
Most people who land on a page like this are dealing with the chronic version. They’ve had a few bad weeks that turned into months, and now they can’t remember the last time they woke up feeling rested.
How Do Stress and Anxiety Affect My Sleep?
Stress is the single most common trigger for why people develop insomnia in the first place. When you’re under stress, your body releases cortisol — a hormone that signals alertness and keeps your nervous system activated. That’s useful at 2pm. At 2am, it’s a problem [4].
The reason this matters is that stress doesn’t have to feel dramatic to disrupt sleep. Low-grade, background worry — the kind you barely notice during the day — can be enough to keep your brain from downshifting into sleep. And once you start losing sleep, the sleep deprivation itself becomes a new stressor, creating a loop that’s genuinely hard to break.
Anxiety disorders make this worse. If you have generalized anxiety, your baseline arousal level is already elevated, which means the threshold for falling asleep is higher than it is for someone without anxiety. The NHS lists anxiety as one of the most common causes of insomnia [2].
In practice this means: if stress or anxiety is your trigger, fixing your sleep schedule alone won’t be enough. You need to address the underlying activation — and that usually means working on the anxiety directly, not just the sleep.
Worth trying if stress is your trigger: A brief “worry dump” journal before bed — write down what’s on your mind and a next action for each item. It sounds simple. It actually helps some people quiet the mental loop enough to fall asleep.
Who Is Most Likely to Develop Insomnia?
Insomnia doesn’t discriminate, but certain groups are significantly more vulnerable. Women are more likely to experience insomnia than men, partly due to hormonal fluctuations across the menstrual cycle, pregnancy, and menopause [8]. Older adults are also at higher risk — sleep architecture naturally shifts with age, and older people spend less time in deep sleep [10].
Other higher-risk groups include:
- People with anxiety or depression
- Shift workers and people with irregular schedules
- Those dealing with chronic illness or chronic pain
- People going through major life changes — job loss, bereavement, divorce
- New parents (situational, but brutal)
It’s not just you. This is one of the most common health complaints worldwide, and the people most affected are often the ones least likely to seek help because they’ve convinced themselves it’s just who they are.
What Medical Conditions Might Be Causing My Sleep Issues?
Several medical conditions directly interfere with sleep, and they’re often missed because people focus on sleep habits rather than underlying health. WebMD and Cleveland Clinic both note that conditions including sleep apnea, restless legs syndrome, chronic pain, acid reflux, asthma, and thyroid disorders are among the most common medical drivers of insomnia [3][10].
Key medical causes to consider:
- Obstructive sleep apnea — you may not know you have it; a partner noticing snoring or gasping is a clue
- Restless legs syndrome — uncomfortable sensations in the legs that worsen at rest
- Thyroid disorders — both hyperthyroidism and hypothyroidism affect sleep
- Chronic pain — arthritis, fibromyalgia, back pain
- Acid reflux (GERD) — lying down worsens symptoms and disrupts sleep
- Neurological conditions — Parkinson’s disease, Alzheimer’s, and others affect sleep regulation [3]
If you’ve tried improving your sleep habits and nothing has changed, this is the category worth investigating with a doctor. A blood panel and a conversation about symptoms can rule out a lot.
If you’re unsure whether your symptoms point to something more serious, it may help to start with a structured self-assessment. This free insomnia test asks about your experience over the past two weeks and can help clarify the pattern — it’s anonymous and takes only a few minutes.
What Medications Could Be Disrupting My Sleep Patterns?
Many common medications list insomnia as a side effect, and it’s one of the most overlooked causes of sleep problems. If your sleep got worse around the time you started a new medication, that’s not a coincidence worth ignoring.
Medications commonly associated with sleep disruption include [1][7]:
- Antidepressants — particularly SSRIs and SNRIs, especially when taken in the evening
- Beta-blockers — used for blood pressure and heart conditions; can suppress melatonin
- Corticosteroids — prednisone and similar drugs are notorious for causing insomnia
- Stimulant medications — ADHD medications like Adderall and Ritalin
- Decongestants — pseudoephedrine in cold medicines
- Some blood pressure medications
- Certain asthma medications — theophylline in particular
The fix here is straightforward: talk to your prescribing doctor. Sometimes adjusting the timing of a dose — taking it in the morning rather than evening — makes a significant difference. Don’t stop a prescribed medication without medical guidance.
Can Insomnia Be a Sign of Depression or Mental Health Problems?
Yes — and this is one of the most important things to understand about sleep disorders. Insomnia and depression have a bidirectional relationship, meaning each can cause or worsen the other [4][7].
About 75% of people with depression report sleep disturbances, according to research cited by Harvard Health [7]. But insomnia can also precede depression — chronic sleep deprivation increases the risk of developing a depressive episode. So asking “why do I have insomnia” sometimes leads to an answer that has more to do with mental health than sleep itself.
Signs that mental health may be the primary driver:
- Waking very early in the morning and being unable to return to sleep (common in depression)
- Persistent low mood, loss of interest, or hopelessness alongside the sleep problems
- Racing, intrusive thoughts at bedtime that feel uncontrollable
- Sleep problems that began during or after a significant emotional event
If this resonates, addressing the mental health piece directly — through therapy, medication, or both — often improves sleep more than any sleep-specific intervention. This is also where CBT-I (Cognitive Behavioral Therapy for Insomnia) overlaps with general CBT for anxiety and depression.
Can Diet and Exercise Help With My Sleep Problems?
Diet and exercise both affect sleep quality, though not always in the ways people expect. Regular physical activity is one of the more consistently supported lifestyle interventions for insomnia — but the timing matters [5].
Exercise earlier in the day tends to improve sleep. Vigorous exercise within two to three hours of bedtime can raise core body temperature and cortisol levels, which delays sleep onset for some people. If you’re exercising late because it’s the only time you have, it may still be worth it — the overall sleep benefit often outweighs the timing issue, but it varies by person.
On the diet side:
- Caffeine has a half-life of about five to six hours, meaning a 3pm coffee still has half its caffeine in your system at 8pm [5]
- Alcohol helps people fall asleep faster but fragments sleep in the second half of the night — you wake more, dream less, and feel worse in the morning
- Large meals close to bedtime can worsen acid reflux and raise body temperature, both of which disrupt sleep
- Magnesium — some evidence suggests it supports sleep, particularly in people who are deficient; worth discussing with a doctor before supplementing
For more on what’s actually disrupting your sleep, this breakdown of the most common sleep culprits covers the lifestyle factors in more detail.
Are There Natural Remedies That Actually Work for Sleeplessness?
Some natural approaches have decent evidence behind them; others are mostly marketing. Here’s what the research actually says, without the wellness fluff.
Has reasonable evidence:
- CBT-I — the most effective non-drug treatment for chronic insomnia; not a supplement but worth naming here [7]
- Melatonin — most useful for circadian rhythm issues (jet lag, shift work, delayed sleep phase) rather than general insomnia; low doses (0.5–1mg) are often more effective than high doses
- Magnesium glycinate — some evidence for improving sleep quality, particularly in older adults
- Relaxation techniques — progressive muscle relaxation, slow breathing; modest but real effect on sleep onset
Limited or mixed evidence:
- Valerian root — studies are inconsistent
- Lavender aromatherapy — may reduce anxiety slightly; unlikely to fix structural insomnia
- Chamomile tea — mild relaxation effect, probably more ritual than pharmacology
This is what worked for me, at least partially: combining a consistent wake time (non-negotiable, even on weekends) with a wind-down period that has no screens and no decisions. Not glamorous. Not a supplement. Just structure.
For a broader look at methods that have real-world backing, this guide to falling asleep faster covers techniques worth trying.
Is Chronic Insomnia Dangerous for My Health?
Chronic insomnia isn’t just unpleasant — it carries measurable health risks. Persistent sleep deprivation is associated with increased risk of cardiovascular disease, type 2 diabetes, obesity, weakened immune function, and mental health disorders [4][10].
The Cleveland Clinic notes that people with chronic insomnia are at higher risk for anxiety, depression, and substance use problems — often because people self-medicate with alcohol or sedatives [10]. Long-term, that creates new problems on top of the original one.
The reason this matters isn’t to scare you. It’s to make the point that insomnia is worth taking seriously as a health issue — not just a lifestyle inconvenience. If you’ve been white-knuckling through years of bad sleep and telling yourself it’s fine, it probably isn’t fine.
What Are the Biggest Mistakes People Make When Trying to Fix Their Sleep?
Most people who struggle with sleep make the same handful of errors. Knowing them doesn’t make them easy to avoid, but it helps.
- Spending too much time in bed — lying in bed awake trains your brain to associate the bed with wakefulness. If you can’t sleep after about 20 minutes, get up.
- Inconsistent wake times — sleeping in on weekends feels good but disrupts your circadian rhythm for the whole week
- Using alcohol as a sleep aid — it works short-term and makes things worse long-term
- Catastrophizing sleep — the more you monitor and worry about sleep, the harder it becomes; the anxiety about not sleeping is often as disruptive as the original trigger
- Trying every new supplement without addressing the root cause — supplements don’t fix structural insomnia
- Ignoring the possibility of a medical cause — especially sleep apnea, which is significantly underdiagnosed
For a deeper look at what might be keeping you up, this article on surprising reasons you can’t sleep covers some of the less obvious ones.
How Do I Know If I Need to See a Sleep Specialist?
You should consider seeing a sleep specialist — or at minimum your primary care doctor — if insomnia has lasted more than four weeks, is significantly affecting your daytime functioning, or hasn’t improved with basic behavioral changes [1][2].
Specific signs you need professional help:
- You suspect sleep apnea (snoring, gasping, waking unrefreshed despite adequate time in bed)
- Your sleep problems began with or are accompanied by significant mood changes
- You’re relying on sleep medications or alcohol regularly
- You’ve had insomnia for more than three months
A sleep specialist can order a sleep study (polysomnography) if a sleep disorder is suspected, and can refer you for CBT-I, which has stronger long-term outcomes than medication for most people with chronic insomnia [7].
If you’re not sure where to start, a structured self-assessment can help you organize your symptoms before a doctor’s appointment. This free, anonymous insomnia test evaluates how you’ve been feeling over the past two weeks and can give you a clearer picture of what you’re dealing with.
How Much Does Insomnia Treatment Typically Cost?
Treatment costs vary widely depending on the approach. Here’s a rough breakdown for 2026:
| Treatment | Estimated Cost |
|---|---|
| GP/primary care visit | $0–$250 (varies by insurance) |
| Sleep study (polysomnography) | $1,000–$3,500 (often covered by insurance) |
| CBT-I with a therapist | $100–$250 per session; 6–8 sessions typical |
| Digital CBT-I programs | $30–$100 total |
| Online therapy platforms | $40–$100/week |
| Prescription sleep medication | $10–$100/month depending on drug and coverage |
| Melatonin/supplements | $10–$30/month |
The honest version is that CBT-I is cost-effective over time because it produces lasting results without ongoing medication costs. Many insurance plans now cover it, and digital CBT-I programs have made it more accessible than it used to be.
Conclusion: Start With Your Trigger, Not a Generic Fix
If you’ve been asking “why do I have insomnia” for months without a clear answer, the most useful thing you can do right now is get specific. Not “I sleep badly” — but when does it happen, what was going on when it started, what makes it worse, and what (if anything) makes it better.
Keep a sleep diary for two weeks. Note bedtime, wake time, how long it took to fall asleep, any wake-ups, what you ate and drank, your stress level, and any medications. Patterns will emerge. They almost always do.
From there, match your trigger to the right intervention:
- Stress and anxiety → CBT-I, anxiety treatment, behavioral wind-down routines
- Medical condition → see a doctor; treat the underlying condition
- Medication side effect → talk to your prescribing doctor about timing or alternatives
- Circadian disruption → consistent wake time, light exposure management, melatonin for rhythm issues
- Learned insomnia → CBT-I, stimulus control, sleep restriction therapy
You don’t have to fall asleep – you just have to rest. Start there. And if you want a structured starting point before your next doctor’s visit, this free insomnia self-assessment can help you get clearer on what you’re actually dealing with.
For more on what might be driving your sleep problems, Napsology covers insomnia, sleep science, and honest product reviews written by someone who actually deals with this – not a wellness brand selling optimism.
Frequently Asked Questions
Q: Why do I have insomnia even when I’m exhausted?
Being tired and being able to sleep are controlled by different systems. If your arousal system (driven by stress, anxiety, or cortisol) is overactive, it can override even significant sleep pressure. This is called hyperarousal and is a core feature of chronic insomnia.
Q: Can insomnia go away on its own?
Acute insomnia often does resolve once the triggering stressor passes. Chronic insomnia – lasting more than three months – rarely resolves without some form of intervention, because the insomnia itself becomes self-sustaining through anxiety and conditioned wakefulness.
Q: Is it normal to wake up at 3am every night?
Waking in the early hours is common and can have several causes: blood sugar dips, cortisol beginning its natural morning rise, sleep apnea, alcohol consumed earlier in the evening, or anxiety. If it happens consistently, it’s worth investigating rather than accepting as normal.
Q: Does melatonin actually help with insomnia?
Melatonin is most effective for circadian rhythm problems – jet lag, shift work, delayed sleep phase. It’s less effective for general insomnia where the issue is hyperarousal rather than a misaligned body clock. Low doses (0.5–1mg) are generally as effective as higher doses.
Q: How long does it take for CBT-I to work?
Most people see meaningful improvement within four to eight weeks of consistent CBT-I practice. It’s slower than medication in the short term but produces more durable results without dependency.
Q: Can screen time really cause insomnia?
Blue light from screens suppresses melatonin and can delay sleep onset, but the bigger issue is often mental stimulation — engaging content keeps your brain alert when it should be winding down. If you’ve already heard this and it hasn’t helped, you’re probably dealing with a different primary trigger.
Q: What’s the fastest way to fix insomnia?
There’s no fast fix for chronic insomnia. For acute insomnia, addressing the stressor directly and maintaining a consistent sleep schedule is the most effective approach. For chronic cases, CBT-I is the fastest path to lasting improvement — faster than medication over a six-month horizon.
Q: Should I take sleeping pills?
Prescription sleep medications can be appropriate for short-term use, particularly for acute insomnia. For chronic insomnia, most guidelines recommend CBT-I as the first-line treatment because medications don’t address the underlying cause and carry risks of dependency with long-term use [1][7].
References
[1] Insomnia Symptoms & Causes – https://www.mayoclinic.org/diseases-conditions/insomnia/symptoms-causes/syc-20355167
[2] Insomnia – https://www.nhs.uk/conditions/insomnia/
[3] Slideshow Insomnia Medical Causes – https://www.webmd.com/sleep-disorders/ss/slideshow-insomnia-medical-causes
[4] What Causes Insomnia – https://www.sleepfoundation.org/insomnia/what-causes-insomnia
[5] Insomnia – https://www.medicalnewstoday.com/articles/9155
[7] Insomnia A to Z – https://www.health.harvard.edu/diseases-and-conditions/insomnia-a-to-z
[8] Insomnia – https://womenshealth.gov/a-z-topics/insomnia
[10] Insomnia – https://my.clevelandclinic.org/health/diseases/12119-insomnia