Post Disclaimer
This post contains affiliate links. If you buy something through these links, I may earn a small commission at no extra cost to you. Full disclosure.
This article is for informational purposes only and does not constitute medical advice. Always consult a healthcare professional for personal health concerns. Full disclaimer.
Last updated: June 10, 2026
Quick Answer: If you’re lying awake asking why you’re unable to sleep, your body is almost always signaling something — stress, a medical condition, a disrupted internal clock, or a nervous system that’s stuck in high alert. Sleep problems rarely have one single cause. Most of the time, it’s a combination of factors layered on top of each other, and understanding which ones apply to you is the first step toward doing something useful about it.
Key Takeaways
- About 35% of adults experience insomnia symptoms, making it one of the most common health complaints worldwide [1]
- Stress and anxiety are the most frequent triggers — they activate your body’s threat response, which is the opposite of what you need to fall asleep [1]
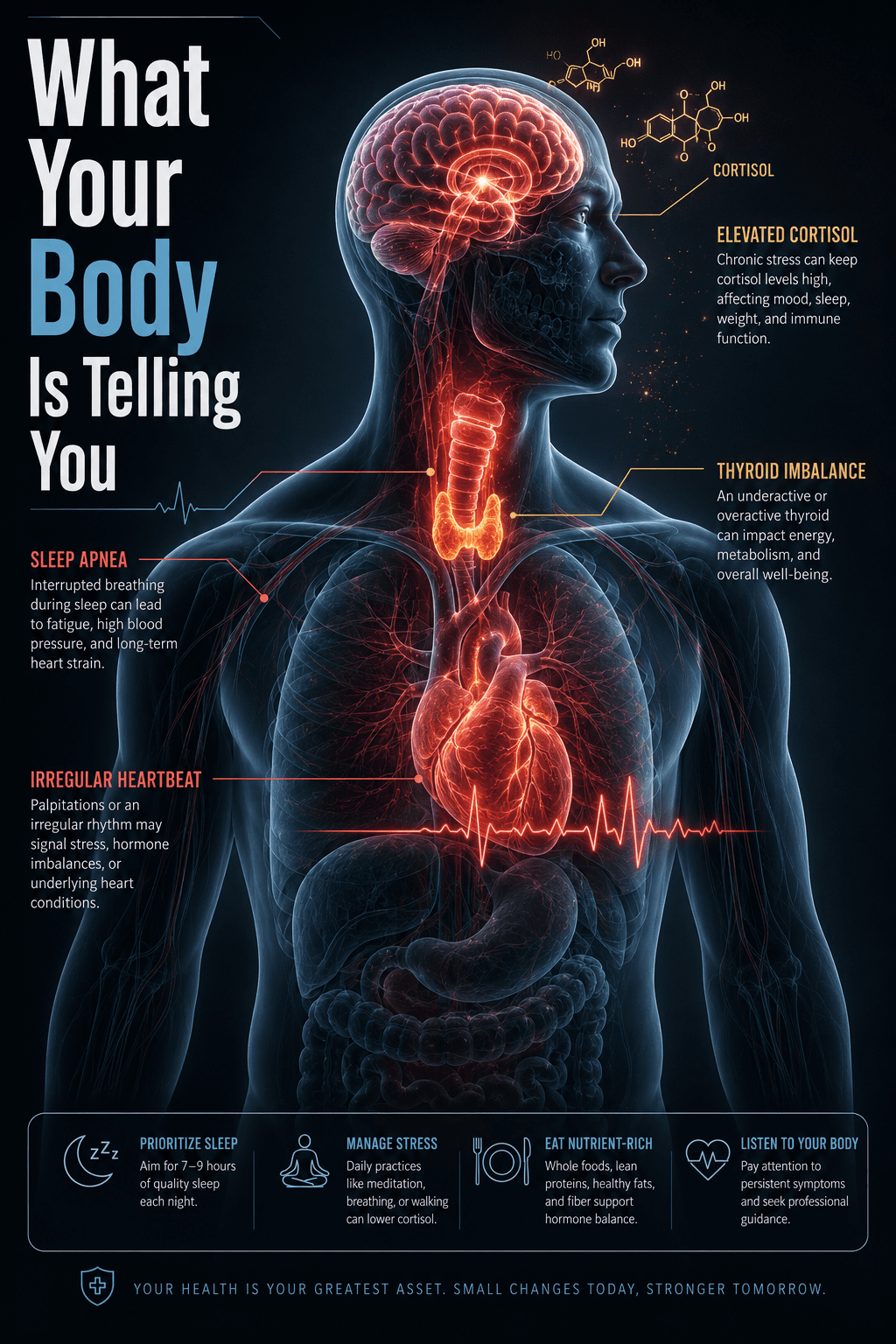
- Medical conditions like sleep apnea, thyroid disorders, and chronic pain are often overlooked causes of poor sleep [5]
- Certain medications — including some antidepressants, blood pressure drugs, and asthma treatments — can directly disrupt sleep [6]
- Hormonal changes (perimenopause, thyroid fluctuations, cortisol dysregulation) affect sleep quality significantly, especially in women
- Sleep needs don’t shrink as much with age as most people think — adults still need 7–9 hours, but the architecture of sleep changes [3]
- Screen use before bed delays melatonin release, but it’s not the only tech habit hurting your sleep
- Natural remedies like magnesium, consistent wake times, and CBT-I have real evidence behind them [9]
- If sleep problems have lasted more than three weeks, a doctor visit is warranted — not optional
- You don’t have to fall asleep — you just have to rest. Removing the pressure to sleep is itself a therapeutic technique
What Are the Most Common Reasons People Can’t Fall Asleep
The most common reasons people are unable to sleep come down to three broad categories: psychological (stress, anxiety, racing thoughts), behavioral (irregular schedules, caffeine, screen use), and physiological (pain, hormones, medical conditions). Most people dealing with chronic sleep problems have at least two of these working against them at the same time [1].
Here’s what the research actually says: insomnia isn’t usually a standalone problem. It’s a symptom. Your brain and body are trying to tell you something is off — and the frustrating part is that figuring out what takes time.
The most frequently reported triggers include:
- Work or financial stress activating the body’s cortisol response at night
- Inconsistent sleep schedules confusing your circadian rhythm [2]
- Caffeine consumed after midday — its half-life is 5–7 hours, meaning a 3pm coffee is still half-active at 8pm [3]
- Alcohol — it helps you fall asleep but fragments the second half of the night [3]
- A sleep environment that’s too warm, too bright, or too noisy
- Underlying anxiety or depression, which are closely linked to insomnia in both directions [4]
If you’ve been dealing with this for a while and the basics haven’t fixed it, the honest version is: basic sleep hygiene was never going to be enough. You need to look deeper.
For a fuller breakdown, this guide to the most common causes of poor sleep covers 10 specific culprits worth working through.
How Do Stress and Anxiety Affect My Sleep Patterns
Stress and anxiety don’t just make you feel worried at bedtime — they physically change what your body does. When your brain perceives a threat (even a financial spreadsheet or a difficult conversation you’re replaying), it triggers the release of cortisol and adrenaline. Those hormones raise your heart rate, sharpen your alertness, and suppress melatonin production [7].
In practice this means your body is doing exactly what it’s designed to do — just at exactly the wrong time.
This state is called hyperarousal. Your nervous system is running a low-grade threat scan even as you’re lying in a dark, quiet room. Researchers have found that people with chronic insomnia often show elevated heart rates and higher cortisol levels at night compared to normal sleepers [7]. It’s not a mindset problem. It’s a physiological one.
Anxiety and insomnia also feed each other. You can’t sleep, so you start to dread bedtime. The dread creates more arousal. The arousal makes sleep harder. This is the cycle that CBT-I (Cognitive Behavioral Therapy for Insomnia) is specifically designed to break — and a 2023 study found it significantly reduces anxiety and improves sleep quality in people with insomnia [9].
If you recognize this pattern, understanding why you can’t sleep even when you’re exhausted might help you name what’s happening.
Is Insomnia a Sign of Something More Serious — and What Medical Conditions Might Be Causing It
Insomnia can absolutely be a sign of something more serious, and this is where a lot of people get stuck — they treat the sleeplessness without investigating what’s underneath it [5].
Medical conditions that commonly disrupt sleep include:
- Sleep apnea — you stop breathing repeatedly during the night, often without knowing it. Loud snoring, waking with headaches, and daytime exhaustion are signs worth checking [5]
- Restless Leg Syndrome (RLS) — an uncomfortable urge to move your legs at night, often worse when lying still
- Thyroid disorders — both hyperthyroidism and hypothyroidism interfere with sleep architecture
- Chronic pain — arthritis, fibromyalgia, and back pain make it physically difficult to stay asleep [5]
- Heart disease and respiratory conditions — these can cause nighttime breathlessness and waking [5]
- GERD (acid reflux) — lying flat worsens symptoms and disrupts sleep more than people realize
- Neurological conditions — including Parkinson’s disease and certain types of dementia
It’s not just you — many people spend years treating insomnia as a standalone problem when there’s an underlying condition driving it. If your sleep problems came on suddenly, or if you wake feeling completely unrefreshed no matter how many hours you get, that’s a signal worth taking to a doctor.
If you’re unsure whether what you’re experiencing qualifies as insomnia, this free and anonymous insomnia test can help you evaluate your symptoms over the past two weeks. It takes a few minutes and asks you to reflect on how you’ve actually been feeling — not just whether you’re sleeping enough.
How Much Sleep Do Adults Actually Need
Adults need 7–9 hours of sleep per night, according to consistent guidance from sleep researchers and organizations including the NIH and the CDC [2]. That range doesn’t shrink much with age — but the structure of sleep does change.
The reason this matters is that many people assume they need less sleep as they get older, or that waking at 4am is just normal. Sometimes it is. But often it’s a sign of disrupted sleep architecture — less time in deep slow-wave sleep, more fragmented REM — not a genuine reduction in sleep need.
A few things worth knowing:
- Short sleepers (people who genuinely function well on 6 hours) exist but are rare — estimated at under 3% of the population
- Sleep debt is real — consistently getting 6 hours when you need 8 accumulates over time and affects cognition, immune function, and mood
- Quality matters as much as quantity — 8 hours of fragmented sleep is not the same as 8 hours of consolidated sleep
If you’re in bed for 8 hours but waking exhausted, the question isn’t how much you’re sleeping — it’s how well.
Can Diet and Exercise Help Me Sleep Better — and What Natural Remedies Actually Work
Diet and exercise genuinely do affect sleep, though the effect size varies by person. Regular moderate exercise has solid evidence for improving sleep quality and reducing the time it takes to fall asleep — but timing matters. Vigorous exercise within 2–3 hours of bed can delay sleep onset for some people [3].
On the diet side:
- Caffeine is the most significant dietary disruptor — its half-life means afternoon consumption still affects nighttime sleep [3]
- Alcohol creates a rebound effect in the second half of the night, reducing REM sleep [3]
- Large meals close to bedtime raise core body temperature and can worsen reflux
- Magnesium (from food or supplements) has emerging evidence for supporting sleep, particularly in people who are deficient
Natural remedies worth trying if you haven’t already:
- Consistent wake time — more powerful than a consistent bedtime, because it anchors your circadian rhythm
- Magnesium glycinate — lower GI side effects than other forms, worth trying if
- CBT-I techniques — sleep restriction, stimulus control, and cognitive restructuring [9]
- Cool bedroom temperature — around 65–68°F (18–20°C) supports the drop in core body temperature that triggers sleep
- Low-light exposure in the evening — not just screens, but overhead lighting too
For practical techniques you can use tonight, these methods for falling asleep faster include options that go beyond the standard advice.
What Medications Might Be Disrupting My Sleep
Several common medications interfere with sleep, and this is one of the most frequently missed causes of insomnia [6]. If your sleep problems started around the time you began a new medication, that’s worth flagging with your prescriber.
Medications known to disrupt sleep include:
- Certain antidepressants — particularly SSRIs and SNRIs, which can suppress REM sleep or cause vivid dreams [6]
- Beta-blockers (used for blood pressure and heart conditions) — reduce melatonin production [6]
- Corticosteroids — cause stimulating effects that interfere with falling asleep
- Decongestants — pseudoephedrine in cold medications is a stimulant
- Some asthma medications — particularly those containing theophylline or albuterol [6]
- Diuretics — cause nighttime urination that fragments sleep
The honest version is: never stop a prescribed medication without talking to your doctor. But do have the conversation. There are often alternatives or timing adjustments that can reduce the impact on sleep.
How Does Age Impact Sleep Difficulties — and Are There Differences Between Male and Female Sleep
Sleep changes with age, and those changes are real — not imagined. Older adults spend less time in deep slow-wave sleep, wake more easily, and experience a shift in circadian timing that makes them feel sleepy earlier and wake earlier [3]. This is normal aging, but it can become problematic when combined with medical conditions, medications, or anxiety about sleep itself.
For women specifically, hormonal fluctuations are a major and underappreciated driver of sleep problems. Perimenopause and menopause bring hot flashes, night sweats, and shifts in estrogen and progesterone that directly affect sleep architecture. Many women in their 40s and 50s find their sleep deteriorates significantly — and it’s not stress, it’s biology.
Men are more likely to develop sleep apnea, which often goes undiagnosed for years. Women with sleep apnea are more likely to be misdiagnosed or dismissed, partly because their symptoms (fatigue, insomnia, mood changes) are less stereotypically “apnea-like” than the loud snoring pattern more common in men.
I’ve noticed in my own experience — and in the conversations I’ve had with readers — that women are more likely to be told their sleep problems are anxiety-related, while men are more likely to have a physical cause investigated first. Both deserve a thorough workup.
What Technology Habits Might Be Ruining My Sleep — and Can Hormonal Changes Cause Sleep Problems
The blue light argument gets most of the attention, but the honest version is that light exposure is only part of the problem with technology and sleep. The bigger issue is mental activation — scrolling social media or reading the news keeps your brain in an engaged, reactive state that’s incompatible with sleep onset [7].
The specific habits that cause the most damage:
- Using your phone in bed — trains your brain to associate the bed with wakefulness (stimulus control is a core CBT-I principle)
- Checking the time repeatedly — increases performance anxiety around sleep
- Bright overhead lighting in the hour before bed — suppresses melatonin as much as screens do
- Working from bed or the bedroom — erodes the mental association between bed and sleep
On hormones: yes, hormonal changes absolutely cause sleep problems, and this is true across the lifespan. Cortisol dysregulation (often from chronic stress), thyroid imbalances, perimenopause, postpartum hormonal shifts, and even testosterone fluctuations in men can all disrupt sleep architecture in measurable ways.
If you’ve been dealing with this for a while and nothing has worked, hormones are worth investigating — especially if your sleep problems came on gradually alongside other symptoms like weight changes, mood shifts, or temperature regulation issues.
If you’re still trying to identify your specific trigger, this guide to finding your insomnia trigger walks through a more systematic approach.
When Should I See a Doctor About My Sleep Problems
You should see a doctor if your sleep problems have lasted more than three weeks, are significantly affecting your daytime functioning, or if you have symptoms that suggest an underlying condition — particularly snoring with gasping, waking with headaches, or unrefreshing sleep regardless of duration.
Don’t wait until you’re desperate. Most people wait far too long.
Specific reasons to seek medical evaluation sooner rather than later:
- You’ve tried consistent sleep hygiene for several weeks and nothing has changed
- You wake up feeling like you haven’t slept even after a full night
- Your partner reports that you stop breathing, gasp, or snore loudly
- You have persistent low mood, anxiety, or concentration problems alongside poor sleep
- Your sleep problems started after a new medication, a major illness, or a significant life event
A GP can rule out medical causes, refer you for a sleep study if needed, and in many cases connect you with a therapist trained in CBT-I — which remains the most evidence-supported treatment for chronic insomnia [10].
If you want to assess your symptoms before that appointment, the free insomnia test here gives you a structured way to evaluate how you’ve been feeling over the past two weeks. It’s anonymous and takes only a few minutes.
FAQ
Q: Why am I unable to sleep even when I’m exhausted?
Exhaustion and sleepiness are not the same state. Chronic stress, hyperarousal, and conditioned wakefulness can keep your nervous system activated even when your body is physically depleted. This is one of the hallmarks of insomnia — the harder you try to sleep, the more alert you become.
Q: Is it normal to wake up at 3am every night?
Waking between 3–4am is common and often linked to the natural lightening of sleep in the second half of the night. But if it happens consistently and you can’t return to sleep, it can indicate depression, cortisol dysregulation, or sleep apnea. Worth investigating if it’s been going on for weeks.
Q: Can anxiety alone cause insomnia?
Yes. Anxiety is one of the most common causes of both sleep onset problems (can’t fall asleep) and sleep maintenance problems (waking in the night). The two conditions reinforce each other, which is why treating anxiety often improves sleep — and vice versa [4].
Q: How long does it take for sleep to improve with CBT-I?
Most people see meaningful improvement within 4–8 weeks of consistent CBT-I practice. It requires effort and temporary discomfort (particularly sleep restriction), but it has stronger long-term outcomes than sleep medication [9][10].
Q: Does melatonin actually work?
Melatonin is most effective for circadian rhythm problems — jet lag, shift work, delayed sleep phase — rather than standard insomnia. It’s not a sedative. Doses above 0.5–1mg are generally no more effective and may cause grogginess the next day.
Q: Can poor sleep cause physical health problems?
Yes. Chronic sleep deprivation is associated with increased risk of cardiovascular disease, type 2 diabetes, immune dysfunction, and impaired muscle recovery. A 2023 study found insomnia increases muscle protein degradation and disrupts muscle clock genes [8].
Q: What’s the fastest way to fall asleep?
There’s no universal answer, but the military sleep method — progressive muscle relaxation combined with mental imagery — has helped many people fall asleep faster. You can find a full breakdown in this guide to the military sleep method.
Q: Should I stay in bed if I can’t sleep?
No. One of the core principles of CBT-I is stimulus control — if you’ve been awake for more than 20 minutes, get out of bed and do something calm in low light until you feel sleepy. Lying awake in bed trains your brain to associate the bed with wakefulness.
Conclusion
If you’re lying awake asking why you’re unable to sleep, you’re not broken and you’re not imagining it. Sleep problems are real, they’re common, and they almost always have a reason — even when that reason takes time to find.
The most useful thing you can do right now is stop treating this as a willpower problem and start treating it as an investigation. Work through the categories: stress and mental health, medical conditions, medications, hormones, habits. Rule things out. Get help when you need it.
A few concrete next steps:
- Track your sleep for one week — note bedtime, wake time, wake-ups, and how you feel. Patterns become visible quickly.
- Check your medications — ask your pharmacist or doctor if anything you’re taking is known to affect sleep.
- Set a consistent wake time and hold it for two weeks, regardless of when you fell asleep.
- Take the free insomnia symptom test if you want a structured way to evaluate what you’ve been experiencing.
- See a doctor if this has been going on for more than three weeks — don’t keep waiting for it to resolve on its own.
You don’t have to fall asleep — you just have to rest. And you don’t have to figure this out alone.
For more on identifying what’s specifically driving your sleep problems, this deep dive into surprising reasons you can’t sleep is worth reading next.
References
[1] What Causes Insomnia – https://www.sleepfoundation.org/insomnia/what-causes-insomnia?utm_source=openai
[2] Causes – https://www.nhlbi.nih.gov/health/insomnia/causes?utm_source=openai
[3] Dsection%3dcauses – https://www.mayoclinic.org/health/insomnia/DS00187/DSECTION%3Dcauses?utm_source=openai
[4] Insomnia – https://www.healthline.com/health/insomnia?utm_source=openai
[5] Causes – https://stanfordhealthcare.org/medical-conditions/sleep/insomnia/causes.html?utm_source=openai
[6] Insomnia Causes – https://www.healthline.com/health/insomnia-causes?utm_source=openai
[7] Insomnia Sleeplessness Anxiety Stress – https://www.nationalgeographic.com/health/article/insomnia-sleeplessness-anxiety-stress?utm_source=openai
[8] arxiv – https://arxiv.org/abs/2312.05033?utm_source=openai
[9] arxiv – https://arxiv.org/abs/2311.09561?utm_source=openai
[10] Index – https://www.healthquality.va.gov/guidelines/CD/insomnia/index.asp?utm_source=openai